Oily skin is a condition characterized by excess sebum production. People affected by oily skin or moderate acne account for about 40-50 % of the population aged 20-40 years old (1). This ‘oily skin’ population is characterized by elevated skin surface lipids (≥ 200 mg sebum/cm2 skin). Excess sebum can lead to discomfort and an unpleasant appearance due to ‘brilliance’ of the skin. It is also a risk factor for the development of skin surface bacterial colonization and inflammation leading to different degrees of acne.
Oily skin is associated with the activity of the pilosebaceus unit in the skin. This unit is composed of a pilosebaceus duct and a sebaceous gland. Features associated with oily skin or moderate acne are: increased sebum production, ductal hypercornification, bacteria colonization of the duct and inflammation (2-3). Sebum production is hormonally controlled, particularly by androgens, but hormones associated with stress also play a major role.
In individuals with oily skin, hyperkeratosis of the follicular epithelium is often linked to abnormalities in lipid composition in the follicle cell membrane (4). These abnormalities lead to barrier dysfunction of the follicle membrane with consequent release of digested lipids, which eventually increase the amount of superficial sebum. A dysfunctional lipid metabolism in the sebaceous gland is responsible for the lack of correct intra- membrane lipid production, with accumulation of free fatty acids and breakdown products (2-4).
It is possible that a local deficiency of certain lipid precursors is associated with this abnormal lipid metabolism in the sebaceous gland of oily skin individuals, with a decreased catabolism of free fatty acids and a slower anabolism and increased breakdown of lipids important for the integrity and functionality of the follicle membrane such as phospholipids, isoprenoids, cholesterol, ceramides, etc. Recent studies have shown that the lack of cholesterol, certain fatty acids, and ceramides are responsible for the membrane barrier disruption of the follicle cell (5). This abnormal lipid metabolism in the pilosebaceous unit would lead to an accumulation of free fatty acids and to a non-functional follicle membrane, resulting in membrane rupture, release of free fatty acids and overall superficial sebum increase.
Based on the hypothesis that oily skin individuals have an altered lipid metabolism of the sebaceous gland due to the lack of lipid precursors, we investigated the role of precursors of pantothenic acid and of farnesyl pyrophosphate (both precursors of lipid metabolism, and in particular of isoprenoid and sterol synthesis) to boost the natural lipid metabolism (increase of free fatty acids catabolism and of isoprenoid and sterol anabolism) in the sebaceous gland with the objective of decreasing free fatty acid accumulation and of increasing follicle membrane lipids. Our ultimate goal was reduction of sebum production and improvement of follicle membrane stability.
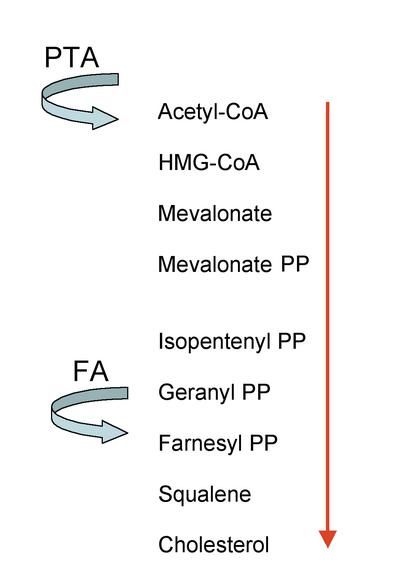
We have synthesized acetylated forms of panthenol and farnesol. These two ingredients are, respectively, panthenyl triacetate (PTA) and farnesyl acetate (FA). They are transformed in the skin to their active forms, PTA to pantothenic acid and FA to farnesyl pyrophosphate. The lypophilic nature of PTA and FA, compared with their more hydrophilic active forms, helps the penetration of the substances through the pilosebaceous unit and therefore increases their availability at the target tissue. Moreover, the molecules transform slowly in their active forms, creating a reservoir for later action. Both PTA and FA are precursors of lipids metabolism, PTA for Coenzyme A and FA for squalene (Figure 1), leading to production of sterols like cholesterol in different tissues including the skin (6-11).
With the goal of decreasing superficial sebum content, we formulated a complex composed of FA and PTA (trade name: Unireduce R-35, Figure 2) and incorporated it at 3% into a low-oil cosmetic emulsion for testing on oily skin volunteers.
Materials and methods
Vehicle and active ingredients (Unireduce R-35)
PTA and FA were synthesized by acetylation of panthenol and farnesol using a proprietary method and incorporated at 3% in a freshly produced cosmetic emulsion with a low fatty acid phase and with no fragrance. Care was taken not to include any potentially skin irritating ingredients.
In vivo study
The subjects were selected from the Derma Consult Concept GmbH (Bonn, Germany) database. They were informed about the importance and meaning of the study. Written informed consent was obtained prior to entry into the trial. The following criteria were used for selection of subjects:
for inclusion in study:
- Female (between 25 and 35 years of age)
- Clinically healthy
- Oily skin (sebum = 200 µg/cm2 skin)
for exclusion from study:
- Skin diseases
- Pregnancy
The subjects of this study were between 25- and 35 years of age (average: 30.4) and had oily skin. They could withdraw from the study at any time without giving any reason. Subjects were instructed not to use any topical preparations on the test areas starting from seven days prior to testing and until the end of the test. For cleansing, only water or a mild syndet (Eubos®; manufacturer: Dr. Hobein, D-53340 Meckenheim-Merl, Germany) was allowed (whole study inclusive of the run-in phase), excluding a period of 12 hours before measurement.
Prior to the first application of the test product, measurements were taken at clearly defined sites on the forehead. One side (randomised) remained untreated and served as control through the study. Further measurements were performed after 14, 28, 42 days of application 8-12 hours following the last daily application (adaptation time: 30 min, room temperature: 21±1°C, relative humidity: 50± 5%) and 2 weeks (day 56) after the last product application. The subjects used the test product (approximately 2 mg/cm2) twice daily (in the morning and evening) in home application after a demonstration in the test institute in a manner corresponding as closely as possible to that to be practised by the consumer.
Measurement of skin surface lipids
Measurements of sebum were performed with the Sebumeter® SM 810 (Courage & Khazaka, Cologne, Germany). The sebum measurement on the skin is based on the world-wide acknowledged Sebumeter method. It is a direct measurement of the sebum secretion on skin. The measurement principle is the photometric method, the grease spot photometer. This method is independent of moisture. A mirror under the measuring section of the tape protruding approximately 1 mm from the measuring head is linked with the cassette by a 0.3 N spring. This makes sure that the tape is pressed onto the measuring area with constant pressure by the mirror. The measuring time of 30 seconds is controlled by a clock in the device. For the determination of sebum, the measuring head of the cassette is inserted into the aperture of the device, where a photocell measures the transparency. The light transmission represents the sebum content on the surface of the measuring area. A microprocessor calculates the result, which is shown on the display in µg sebum/cm2 of the skin. Each value was the average of three measurements.
Statistical analysis
Data were analysed using the Student’s T Test.
Results
In our group sample, measurement of sebum level in the untreated area (that had been randomized through the different subjects) over the experimental period, demonstrated a consistently elevated superficial sebum level during the whole study (see Figure 3). This measurement confirmed that our sample group is indeed suffering from a persistent oily skin condition, unlike subjects with combination skin where fluctuations of skin oiliness are frequent and often associated with hormonal status and environmental conditions.
Treatment with 3% Unireduce R-35 was found to decrease sebum content on the forehead of our oily skin volunteers at all time points tested. Reduction was statistically significant when compared with the untreated area (p < 0.01, Student’s T test) after 28 and 42 days of application (-19.8% at day 42) and on day 56 (14 days after discontinuation of product use) demonstrating that the product had a lasting reduction effect. Table 1 gives details of all the measurements performed, while Figures 3-4 summarize the results.
Finally, the product showed an excellent safety profile. Dermatological tests didn’t show any sign of skin irritation and the product was well tolerated (data not shown).
Discussion and Conclusion
We have investigated the hypothesis that a topical lack of certain precursors of lipid metabolism such as PTA and FA, could lead to excess sebum production in individuals suffering from oily skin condition. Unireduce R-35 (containing PTA and FA) application proved successful in decreasing sebum on the forehead and maintaining a long lasting effect. This long lasting effect could be due to the precursor nature of PTA and FA. These molecules would probably accumulate in the skin, creating a reservoir prior to be slowly converted into their active forms. Skin penetration studies are planned to further investigate this hypothesis.
Unireduce R-35 showed a very high efficacy in decreasing superficial skin sebum content. We achieved almost 20% superficial skin sebum reduction after 42 days treatment, superior to previous attempts such as in the work published by Pierard, G.E. et al, that utilized alternative treatment to fight oily skin (2). We believe that the mechanism of and main reason for this success is the stimulation of free fatty acid catabolism and of isoprenoid/sterol syntheses by PTA and FA.
In the early ’90s, studies from Dr Leung suggested a lack of pantothenic acid as one of the causes of acne (12-13). In fact, this deficiency would account for a reduced Coenzyme A formation (since pantothenic acid is part of Coenzyme A) and therefore reduced lipid metabolism. A clinical study conducted by Dr Leung on 100 people with moderate acne further proved this hypothesis. Subjects supplemented orally with 10 g/day of pantothenic acid in combination with topical application of a cream containing 20% of pantothenic acid showed clear improvement of their condition after only 2-3 days from start of treatment and complete remission after 8 weeks (13). Therefore we can hypothesize a link between pantothenic acid, lipid metabolism and acne condition. More recent clinical studies in healthy subjects treated with a cream containing panthenol, a precursor of pantothenic acid, showed a significant improvement of the epidermal barrier function measured by trans-epidermal water loss, further suggesting a key role for pantothenic acid as a precursor for membrane lipids biosynthesis (14).
Farnesyl acetate is also a precursor of the isoprenoid and sterol syntheses (6) and although there are no clinical studies demonstrating direct involvement of farnesyl acetate in acne conditions or in follicle membrane barrier integrity we can strongly suspect this link. Further studies would be needed to clearly demonstrate this hypothesis.
In conclusion we have demonstrated that Unireduce R-35 is an excellent product for combating oily skin since it significantly decreases superficial sebum content and also possesses long lasting efficacy. We wanted to create a product that unlike previous commercially available oily skin treatments such as salicylic acid- AHA (alpha hydroxy acid)- sulfur- based products, etc (15) was not keratolytic, and does not cause skin dryness or irritation. Unireduce R-35 does not contain any chemical boosters, but is based on derivatives of natural substances, and it does not cause skin dryness, exfoliation or irritation. Unireduce R-35 is particularly indicated for oily skin individuals that seek a mild and natural treatment of their condition and that are particularly sensitive to skin irritants.
Authors
Dr. William McGregor, Dr. Kuno Schweikert
Induchem AG, Industriestrasse 8a,
CH-8604 Volketswil, Switzerland
www.induchem.com
Dr. Giorgio Dell’Acqua (to whom correspondence should
be addressed)
Dellacqua Consulting
Rue Louis Meyer 9D, 1800 Vevey, Switzerland
fax/tel: +41-21-921-3330
e-mail: g.dellacqua@dellacquaconsulting.com
www.dellacquaconsulting.com






